
Institutional Adoption Strategy
The clinical case is solid. The champion believes in it. So why does the committee keep sending them home empty-handed?

Written by
Dale Hogeland . CEO & Founder
Published
There’s a moment I’ve heard described so many times it’s practically a pattern.
A champion walks into a committee meeting feeling as ready as anyone could reasonably expect. They’ve reviewed the data. They know the outcomes cold. They’ve used the product, seen what it does, and they genuinely believe this is the right call for their patients.
And then someone from finance asks a question they didn’t see coming.
Not a clinical question — those they can handle in their sleep.
A reimbursement question.
A workflow question.
Something about storage or chain‑of‑custody.
And the champion — the person who has put real professional credibility on the line — doesn’t have the answer.
The room feels it instantly.
You can almost watch the shift happen.
Confidence dips.
The momentum softens.
And the committee does what committees do when uncertainty walks in the door: they protect the institution.
“Let’s revisit this next quarter.”
That’s not a no.
But it’s not a yes.
And for a lot of products, that quiet deferral is where the adoption timeline starts to unravel.
The champion isn’t failing. They were sent in without the right tools.
This is the part nobody likes to say out loud — and the part that matters most.
Clinical champions are some of the most capable people in the building. They’re not stumbling in these meetings because they don’t understand the product. They’re stumbling because they walked in ready for a clinical discussion and found themselves in a business meeting instead.
Those are two very different rooms.
In a clinical conversation, the logic is shared. You talk about healing curves, wound progression, patient trajectories — and the person across from you tracks every step because they live in the same world.
A committee meeting runs on a different operating system.
The CFO isn’t thinking about wound closure rates. They’re thinking about reimbursement exposure and what happens when a DRG collapses. The nursing director isn’t focused on clinical endpoints. They’re thinking about staffing ratios and what this does to the shift. The value analysis coordinator is thinking six months ahead — about defensibility, documentation, and institutional risk.
The champion is speaking clinical. The room is speaking financial, operational, and institutional.
That disconnect isn’t a communication flaw. It’s a preparation gap — and it’s one almost no company closes before sending their champion into that room.
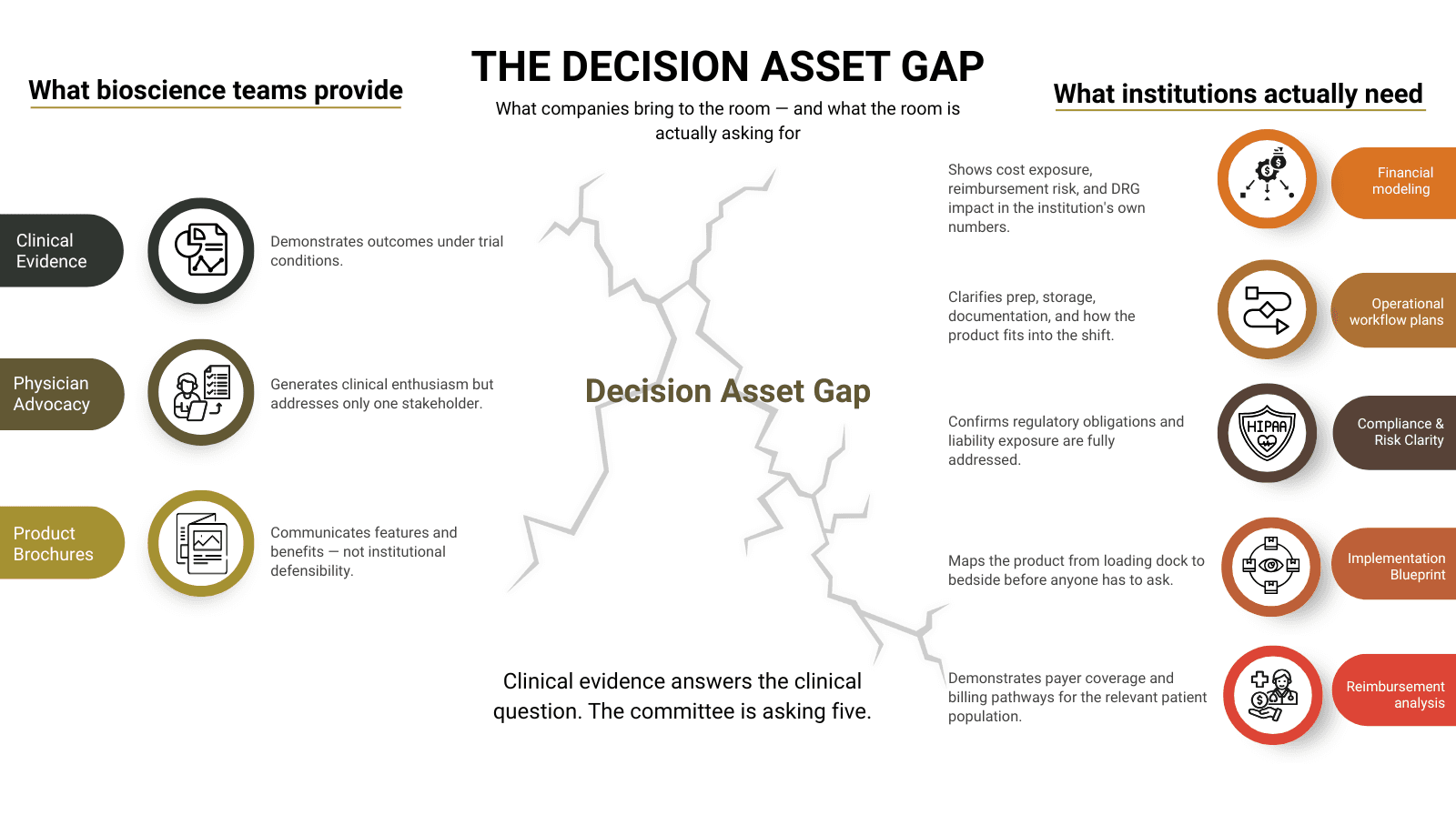
What the room is actually asking
As I wrote in “Why Your Biologic Is FDA Approved but Not Yet Hospital Approved,” adoption rarely stalls because the science is weak. It stalls because the institutional case around that science was never fully built.
Committees aren’t adversaries. They’re people with real accountability — for budgets, for staffing, for what happens if a decision doesn’t go the way anyone hoped. When they ask hard questions, they’re not trying to block the product. They’re trying to protect the institution.
And that’s actually the opening.
Because once you understand what they’re protecting, you can give them what they need to feel safe, so they say yes. The financial story. The operational picture. The answer to the question they haven’t asked yet — but absolutely will.
There are three moments in a committee room where adoption either holds… or quietly breaks.
The financial moment
Someone looks at the price, and the comparison is immediate. Standard of care costs this. Your product costs that.
On the surface, the math feels simple — until you flip it.
What does a readmission actually cost? What does a non‑healing wound cost over 90 days? What happens financially when that patient comes back within 30 days and the reimbursement evaporates?
The champion who can answer those questions using the committee’s own numbers — not industry averages, not brochure language, but the institution’s actual DRG exposure — changes the conversation. The product stops looking like a line item. It starts to look like protection.
The operational moment
Long before the nursing director ever votes, five questions are already circulating quietly: Where does it get stored? How long does prep take? Will it help standardize clinical workflow and care protocols? Will it reduce the contracted price of supplies? — and does it fit into what we’re already running?
If those questions hang unanswered, the floor becomes a quiet no. Not out of resistance — out of self‑protection. And that no travels upward fast. It reaches the committee well before the champion ever opens their slide deck.
The only way to stop that momentum is to answer those questions before they’re asked. A clean, visual picture of how the product fits into the day — prep, workflow, documentation — takes operational anxiety off the table.
The silent moment
This is the one that hits hardest.
The champion is mid‑presentation. The room has been listening. And then a committee member asks the question — about reimbursement coding, or fallback plans if outcomes vary, or what happens to the budget if volume doesn’t materialize the way it was projected.
And the champion doesn’t have a clean answer.
The silence only lasts a few seconds. But everyone in the room feels it. Confidence drops. Momentum drains. And the committee does what it always does in that moment.
It defers.
That silence is where approvals go to die. And it’s entirely preventable.
What changes when the champion is actually prepared
I want to be precise here, because “better prepared” doesn’t mean more slides.
What changes when a champion walks in with the right support isn’t volume. It’s confidence — the quiet, grounded kind that comes from knowing which questions are coming and having clear, honest answers ready.
They don’t tense up when finance pushes back, because the CFO‑Ready Summary has already translated clinical value into the institution’s own numbers. They don’t hesitate when operations weigh in, because the Workflow Map has already shown how the product fits into the shift. They don’t go quiet when the room gets hard, because the Rebuttal Guide has already given them the language — not a script, just a few sentences that keep the conversation moving.
I’ve heard this described as the difference between defending a product and guiding a decision.
When a champion walks in exposed — answering from memory, hoping the clinical story carries the room — they’re defending. It’s reactive. It’s draining. And it puts an unfair amount of pressure on one person who was never meant to carry the institution’s entire decision logic alone.
When the champion is prepared, something else happens. They’re not trying to convince anyone. They’re walking the room of smart, cautious people through a decision those people already want to make — if someone can give them the clarity to do it safely.
That’s what the Committee Survival Kit is built to do. Not to sell the product. Not to overwhelm the committee with evidence. Just to give the champion footing instead of exposure.
The CFO‑Ready Summary So the price stops being the headline and starts being the protection.
The Budget Impact Model So the conversation shifts from what it costs to what it saves — in their numbers, not yours.
The Operational Workflow Map So the floor stops imagining disruption and starts seeing how the product fits into the day.
The Champion’s Rebuttal Guide The quiet confidence they reach for when the room goes still, and all eyes turn to them.
The Implementation Blueprint Proof that the hard parts have already been thought through — before the committee asks.
Peer Benchmarking So the committee knows they’re not the first to move — and won’t be the last.
None of these tools make the decision for the committee. They simply make the decision possible.
What nobody tells you about the champion
Here’s the piece I keep coming back to.
When a champion walks into that room without the right support, they’re not just representing themselves. They carry the company’s science, the company’s economics, and the company’s operational story — all at once. They’re not in the room with backup.
They are the backup.
And they’re often the only person in that room who is thinking about the patient first.
That’s a lot of weight for one person to carry.
The companies I see struggling with institutional adoption — watching the same product stall at the same committee for the third or fourth quarter in a row — usually aren’t failing on clinical evidence. They’re failing on that weight. They’ve placed everything on the champion and given them very little to carry it with. A cross they shouldn’t have to bear.
If your champion keeps walking out of that room without a yes, it’s worth asking whether the problem is really the committee — or whether the champion was sent in without the footing they needed.
That’s the question the Audit is built to answer.
Also in this series:
Part 1: Why Your Biologic Is FDA Approved but Not Yet Hospital Approved
Part 3: The Committee Isn’t Trying to Block You
The ClearSignal Clarity & Adoption Audit™ identifies exactly where adoption is breaking down — and what needs to be in your champion’s hands before the next committee meeting. If you’re ready to see what’s really happening inside those rooms — and what it would take to change the outcome — the Audit is where we start.
Dale Hogeland is the Founder & CEO of ClearSignal, a decision enablement and adoption strategy consultancy for commercial-stage wound care biologics and regenerative bioscience companies. He spent 15 years as an acute dialysis nurse and a VNA wound care nurse before building ClearSignal to help commercial teams give their champions the internal footing they need to carry an approval across the line.
References
1. Institute for Healthcare Improvement. Value Analysis Committees and Technology Assessment in Health Systems.
2. Healthcare Financial Management Association. Technology adoption and value analysis in modern health systems.
3. Burns LR, Bradley EH, Weiner BJ. Shortell and Kaluzny’s Healthcare Management: Organization Design and Behavior.
4. Greenhalgh T et al. Diffusion of Innovations in Health Service Organizations. Milbank Quarterly.

Institutional Adoption Strategy
Why Your Biologic Is FDA Approved but Not Yet Hospital Approved

Institutional Adoption Strategy
The Committee Isn’t Trying to Block You

Institutional Adoption Strategy
What The 2026 Medicare Financial Reset Means To Advanced Tissue Bioscience Companies... And What To Do About It.