
Institutional Adoption Strategy
Your science is solid. Your clinical champion is ready. So why does the committee keep deferring?

Written by
Dale Hogeland . CEO & Founder
Published
You’ve probably seen this play out.
Clinicians are excited. The data looks good. Everyone agrees the science makes sense.
And then… nothing moves.
The technology sits in review. Committees keep deferring.
FDA approval was hard. Hospital approval is the part nobody prepared you for.
Meanwhile, patients who could benefit are waiting — and your commercial timeline keeps slipping.
Out in the field, I kept seeing the same thing: strong products, clinicians ready to move… and everything still stalling because the people making the call didn’t have the internal backup to stand behind it.
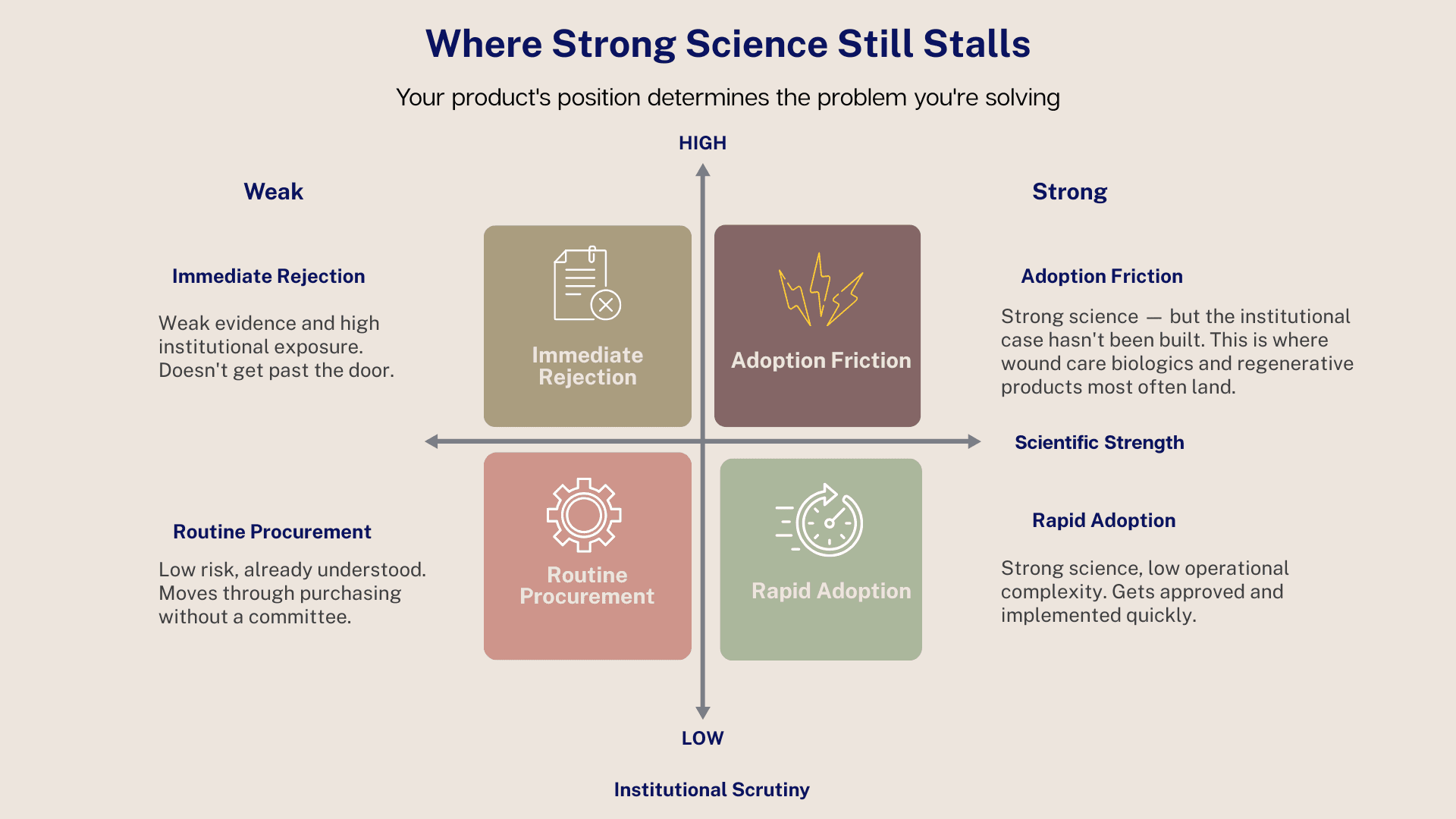
Here’s the part most teams don’t realize: the holdup usually isn’t the clinical story. It’s the internal risk your champions are being asked to carry.
The Guessing Game That Costs You the Room
When adoption slows, teams usually start guessing at the obvious stuff — maybe they need more data.
Maybe physicians haven’t heard enough about it.
Maybe the hospital just isn’t ready for something new.
All fair thoughts, but they miss what’s actually happening inside the system.
Within a health system, new technologies aren’t judged by their excitement. They’re judged on whether the people responsible can defend the decision if someone pushes back.
If that internal defense feels shaky, even slightly, the safest move is to pause. Not because the evidence isn’t there. Because the internal case isn’t clear enough yet.
The Three Boulders Nobody Warned You About
Most products don’t stall because of the science. They stall because the CFO can’t see the financial upside, the floor can’t see how it fits into their shift, and the committee can’t see why changing the status quo is worth the risk. Clear those three friction points — what I call the Institutional Boulders — and adoption moves.
Boulder 1 — Financial Risk: The CFO’s Wall
I used to hear this from commercial teams all the time — “We’re getting killed on price.” But here’s the thing nobody tells you: committees almost never kill a product because of the number itself. They kill it because they don’t understand what that number protects them from.
Sometimes, the part that commercial teams don’t realize is this: the financial case isn’t fully calculated on their side. The clinical data is solid — efficacy, outcomes, wound‑closure rates — but the Total Cost of Care analysis showing what your product actually saves the hospital hasn’t been built yet. Not because anyone ignored it, but because that kind of math requires a different lens. It takes someone who understands both the reality of the clinical floor and the way a hospital’s financial structure works — and can connect the two.
When that analysis is missing, your reps walk into a room with clinical evidence and no economic translation. They don’t know what they don’t know. And neither does the committee.
From your side, you may not realize your biologic prevents a $45,000 readmission. Nobody has run that calculation. So instead of reframing the $3,000 line item, your champion ends up defending it — and losing ground in a conversation that was never actually about the price.
And that’s the real issue.
Hospitals don’t make decisions based on clinical excitement — they make decisions based on whether the person signing off can defend that decision if someone pushes back. If the financial story isn’t crystal clear, the safest move in the room is always to pause.
It’s not that your price is wrong. It’s that the value hasn’t been framed in the language they use to protect the institution.
Once you show them their own DRG math — their penalties, their cost of complications, their length-of-stay exposure — the conversation changes. Suddenly it’s not, “Why is this so expensive?” It becomes, “Why would we keep paying for avoidable risk?”
That’s the shift. You’re not fighting a pricing problem. You’re fighting a framing problem.
Boulder 2 — Operational Anxiety: The Floor’s Resistance
When clinicians love your product, but it still keeps stalling, it’s almost always because the people who have to live with it day-to-day can’t yet see how it fits into their world. And I say that as someone who’s been that nurse.
When I was doing VNA wound care, the decision about a new product didn’t start in the patient’s home — it started back at the office. If the operational picture wasn’t clear before it ever hit my bag — how it was stored, how it was prepped, what the documentation looked like — it never made it into the field. Not because it wasn’t good, but because nobody had built the workflow around it. And without that, it was safer to stick with what we already knew worked.
Hospitals and clinics are no different.
If the operational details aren’t nailed down — storage, prep, workflow, documentation — the floor becomes a quiet no. Not out of resistance, but out of self-protection. And that quiet no travels upward fast. It reaches the committee long before your champion ever gets a chance to make their case.
So, when you see a product with strong clinical support and excited clinicians still getting stuck, it’s almost always because the people responsible for using it can’t yet picture how it fits into the shift. Until that’s solved, nothing moves.
Boulder 3 — Clinical Inertia: The Status Quo Is Free
Clinical Inertia is the toughest and quietest of the three boulders. It catches most teams off guard — not because committees are stubborn or skeptical of the science, but because the status quo feels safe.
The Financial Boulder has numbers you can reframe. The Operational Boulder has a workflow you can fix. But Clinical Inertia? That’s psychology. That’s institutional muscle memory.
From the committee’s side of the table, the current standard of care is the devil they know. It’s already budgeted, already trained for, and already defended. Everyone knows how to use it, how to chart it, and how to justify it if something goes sideways. It may not be perfect, but it’s familiar — and familiar feels safe.
So when you bring in something new, you’re not just asking them to adopt a better option. You’re asking them to take on new risk — clinical, financial, operational, reputational — and to take responsibility for that.
That’s Clinical Inertia. It’s not resistance — it’s institutional self-preservation. And until you show them, in their language, why change is actually safer than staying where they are, “not right now” will always be the easiest decision in the room.
The Champion Carries More Than You Know
When a clinical champion walks into a VAC room without the right support, it’s not a debate — it’s an ambush. They’re the one person in the room who cares about the patient first, and they’re surrounded by people who are paid to care about everything else.
Most champions think they’re walking into a clinical conversation. They’re not. They’re walking into a business meeting where they’re the only clinician in the room.
The committee isn’t trying to block them — they’re trying to protect the institution. Those two realities collide in real time.
And here’s the part that hits hardest: the champion isn’t just presenting their case — they’re carrying your case. The company’s science, the company’s economics, the company’s operational story… alone.
They’re not in the room with backup. They are the backup.
What Changes When the Champion Is Prepared
When a champion walks into that room with the right support, the whole energy shifts. They’re not guessing. They’re not hoping the committee “gets it.” They’re carrying a story that actually holds up under pressure.
It doesn’t make the meeting easy. It just makes it fair.
A prepared champion isn’t trying to convince anyone. They’re guiding the room through a decision the committee can stand behind. They’re not defending a product — they’re defending a plan.
And that’s where the Committee Survival Kit comes in. It’s ClearSignal’s answer to that preparation gap — six decision assets built specifically to give your champion the footing they need before they ever walk into that room. Not slides. Not templates. Not marketing material dressed up as strategy. Each tool addresses a specific moment where adoption either holds or breaks.
The CFO-Ready Summary — the piece that lets your champion walk in speaking finance instead of hoping finance meets them halfway.
The Budget Impact Model — the moment the conversation shifts from “What does it cost?” to “What does it save us?” — in their numbers, not yours.
The Operational Workflow Map — the point where the floor stops imagining chaos and starts seeing how the product actually fits into their day.
The Champion’s Rebuttal Guide — the quiet confidence in their back pocket — the three sentences that keep the room from drifting back to “not right now.”
The Implementation Blueprint — proof that you’ve already thought through the hard stuff before the committee even asks.
Peer Benchmarking — the reassurance every committee needs: proof they’re not the first to take the leap… and won’t be the last.
None of these tools make the decision for the committee — they simply make the decision possible.
This Is What Hospital Approved Actually Looks Like
Everything in this article comes down to one simple idea: your product doesn’t need louder marketing — it needs clearer pathways through the places where adoption actually breaks down.
When the financial story lands, when the operational picture is clear, when the champion walks in prepared instead of exposed… that’s when a product becomes Hospital Approved. Not because the science changed, but because the institution finally had what it needed to say yes.
And that’s why the first step isn’t a deck, a toolkit, or a campaign. It’s clarity.
The ClearSignal Clarity & Adoption Audit™ is where we start — a low-lift, high-signal look at the three boulders standing between your product and institutional approval. No pressure. No commitment. Just the truth about what’s slowing you down and what it will take to move forward.
If you’re ready to see what’s really happening inside those rooms — and what it would take to change the outcome — the Audit is the cleanest way in.
Also in this series:
Part 2: The Champion Is Ready. The Room Isn’t.
Part 3: The Committee Isn’t Trying to Block You
The ClearSignal Clarity & Adoption Audit™ identifies exactly where adoption is breaking down — and what needs to be in your champion’s hands before the next committee meeting. If you’re ready to see what’s really happening inside those rooms — and what it would take to change the outcome — the Audit is where we start.
Dale Hogeland is the Founder & CEO of ClearSignal, a decision enablement and adoption strategy consultancy for commercial-stage wound care biologics and regenerative bioscience companies. He spent 15 years as an acute dialysis nurse and a VNA wound care nurse before building ClearSignal to help commercial teams give their champions the internal footing they need to carry an approval across the line.
References
Institute for Healthcare Improvement. Value Analysis Committees and Technology Assessment in Health Systems.
Healthcare Financial Management Association. Technology adoption and value analysis in modern health systems.
Burns LR, Bradley EH, Weiner BJ. Shortell and Kaluzny’s Healthcare Management: Organization Design and Behavior.
Greenhalgh T et al. Diffusion of Innovations in Health Service Organizations. Milbank Quarterly.


