
Institutional Adoption Strategy
They’re trying to protect something. Once you understand what that is, the whole strategy changes.

Written by
Dale Hogeland . CEO & Founder
Published
Think about what a Value Analysis Committee member has actually lived through.
They’ve seen innovations arrive with strong clinical evidence. Physician champions who believed in them deeply. Commercial teams were convinced this one was finally going to move fast.
Some of those products delivered exactly what was promised. Others didn’t — and when things went sideways, it wasn’t the sales team who had to explain the decision.
It was the committee member.
To administration. To finance. Sometimes to patients.
That experience doesn’t make them resistant. It makes them careful. And from the outside — especially when you’re waiting on a yes — careful can look a lot like obstruction.
But here’s what changes when you stop reading the committee as an obstacle and start reading them as a room full of people trying to protect something real.
You stop pushing against them. And you start building toward them.
The entire strategy shifts.
The committee isn’t trying to slow down your timeline. They’re trying to protect their institution. Those are very different problems to solve.
What they’re actually protecting
A Value Analysis Committee isn’t a single point of view. It’s a group of people with very different responsibilities sitting in the same room — each one looking at your product through a completely different lens.
The clinical representatives are asking whether the evidence is strong enough to justify change, and whether outcomes will hold up outside of trial conditions. That’s the lens most commercial teams prepare for — and they’re right to. Clinical scrutiny is real.
But it’s rarely where adoption actually breaks.
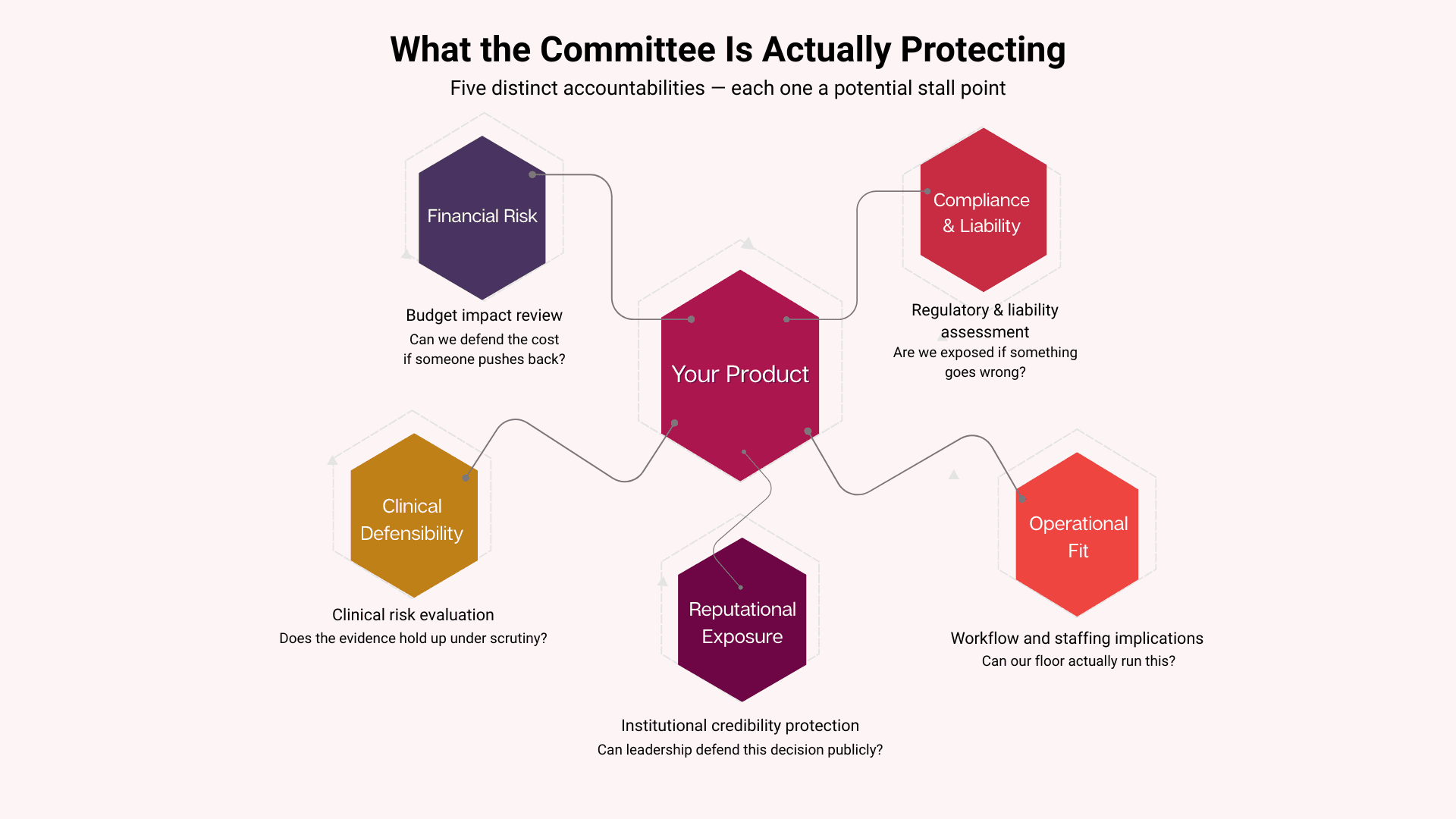
The financial representatives are asking a different set of questions entirely. Not does this work, but what does adoption really cost us.
Total cost, not unit price.
Does the reimbursement pathway hold? If volume comes in lower than projected, does the math still work? If outcomes vary in a subset of patients, what’s the financial exposure?
The operational voices — nursing leadership, supply chain, pharmacy — are thinking about everything the data doesn’t show. Where does it live? What does it add to the shift? Who owns the documentation, and does it fit into the systems already in place? They’re not being difficult. They’re trying to picture implementation before the institution commits — because they’re the ones who will live with the consequences.
And then there are the people who aren’t in the room at all.
The billing coder who has to make sense of something that doesn’t fit cleanly into an existing code. The risk manager who needs to understand liability if outcomes vary. The compliance officer, who has to confirm there are no documentation gaps that create regulatory exposure.
None of them vote. All of them can quietly stop adoption long before a decision is ever formalized.
As I described in “Why Your Biologic Is FDA Approved but Not Yet Hospital Approved,” these pressures show up as the Three Boulders — financial risk, operational anxiety, and clinical inertia. But understanding them as boulders is the company’s job.
Understanding them as the things the committee is trying to protect is what changes the posture.
Every hard question in that room is someone protecting something they are accountable for. The question isn’t how to neutralize that — it’s how to honor it.
The two kinds of submissions
After enough time in these rooms, a pattern becomes hard to ignore. You start to see why some submissions move — and why others quietly stall.
The first kind is familiar. The clinical story is strong and well told. The evidence is organized. The physician champion is credible and engaged. And then the first non‑clinical question lands — about reimbursement, or workflow, or implementation — and the answer isn’t ready.
The committee doesn’t reject it. They defer. They ask for more information. They are scheduled for another meeting.
And that cycle repeats. Quarter after quarter. Until the momentum simply fades.
That’s not a product failure. It’s a preparation failure.
The second kind feels different the moment it enters the room.
The financial picture is already grounded in the institution’s own numbers — not industry benchmarks, not brochure language, but real cost exposure. The operational story is visible before anyone asks — where it lives, how it’s prepped, what documentation it requires. The champion can answer the hard questions not because they’re improvising, but because those answers were built long before the meeting.
The committee still asks questions. But they land differently when the answers are already there. Instead of surfacing gaps, the questions confirm readiness. And a committee that feels prepared to defend a decision moves very differently than one still searching for clarity.
This is what the second article in this series explored in detail — what the champion needs to carry into that room, and why the tools matter as much as the person holding them. Preparation isn’t about making the champion smarter. It’s about making the decision defensible before anyone has to defend it.
The committee wants to say yes
This is the part that often gets lost once adoption stalls and frustration sets in.
Committees aren’t trying to run out the clock on your product. They’re not philosophically opposed to innovation. Most of them have watched promising treatments sit on the shelf longer than they should have — and felt the frustration of that firsthand.
They know what slow adoption costs. In patient outcomes. In institutional credibility. In the growing gap between what medicine can do and what medicine is actually doing.
They want to say yes. What they can’t do is say yes without being able to defend it.
Inside a healthcare institution, defending a decision means being able to answer in three directions at once.
Upward — to administration and finance.
Sideways — to the departments that will carry the operational impact.
Downward — to the clinicians whose daily work changes the moment adoption happens.
If even one of those conversations can’t be held with confidence, the safest move is to wait.
Not because waiting is good.
Because uncertainty is worse.
The committee’s default answer isn’t no. It’s “not yet.” The difference between those two outcomes is almost always the quality of the case that was built before the meeting.
What it means to build toward the committee
Something shifts when commercial teams really internalize this.
The old posture is adversarial — even when it doesn’t feel that way. It sounds like: we have strong evidence, we have physician support, we just need to get this through the committee. The committee becomes the final obstacle between the product and the market. The goal is to overcome resistance.
That posture produces the wrong kind of submission. It optimizes clinical persuasion and treats financial, operational, and institutional questions as objections to manage — rather than as legitimate concerns to address.
The new posture is collaborative.
It starts with a different assumption: the committee has real accountability. They will be asked to defend this decision. The job isn’t to push past them — it’s to make that defense possible. To give every person in the room what they need to feel confident saying yes and protected if anything goes sideways afterward.
That posture creates a different kind of submission. Not louder. Not longer. Not more clinical. Just more complete. More honest about the operational reality. More specific about the financial story. More prepared for the questions that were always going to come.
It’s the difference between walking in to convince — and walking in to equip.
And committees feel that difference immediately.
The question worth asking before the next meeting
When a product has been sitting in committee review longer than the commercial timeline can absorb, the instinct is usually the same.
Revisit the clinical story. Add more data. Bring in more physician voices. Push harder on efficacy.
But if the clinical case was already solid — and for most commercial‑stage wound care biologics and regenerative bioscience products, it is — more evidence rarely moves the timeline.
The more useful question is a different one.
Not: Is our evidence strong enough?
But: Have we given the committee everything they need to defend a… yes?
The financial story in their numbers.
The operational picture, their floor can actually see.
The answers to the questions that will come from billing, compliance, and risk — before those questions slow the process down.
And for the champion carrying it in, the footing to hold the room steady when it gets hard.
That’s the case the committee needs. Not a stronger clinical argument. A complete institutional one.
Also in this series:
Part 1: Why Your Biologic Is FDA Approved but Not Yet Hospital Approved
Part 2: The Champion Is Ready. The Room Isn’t.
The ClearSignal Clarity & Adoption Audit™ identifies exactly where adoption is breaking down — and what needs to be in your champion’s hands before the next committee meeting. If you’re ready to see what’s really happening inside those rooms — and what it would take to change the outcome — the Audit is where we start.
Dale Hogeland is the Founder & CEO of ClearSignal, a decision enablement and adoption strategy consultancy for commercial-stage wound care biologics and regenerative bioscience companies. He spent 15 years as an acute dialysis nurse and a VNA wound care nurse before building ClearSignal to help commercial teams give their champions the internal footing they need to carry an approval across the line.
References
1. Institute for Healthcare Improvement. Value Analysis Committees and Technology Assessment in Health Systems.
2. Healthcare Financial Management Association. Technology adoption and value analysis in modern health systems.
3. Burns LR, Bradley EH, Weiner BJ. Shortell and Kaluzny’s Healthcare Management: Organization Design and Behavior.
4. Greenhalgh T et al. Diffusion of Innovations in Health Service Organizations. Milbank Quarterly.
5. Balas EA, Boren SA. Managing Clinical Knowledge for Health Care Improvement. Yearbook of Medical Informatics. 2000.

Institutional Adoption Strategy
Why Your Biologic Is FDA Approved but Not Yet Hospital Approved

Institutional Adoption Strategy
The Champion Is Ready. The Room Isn’t.

Institutional Adoption Strategy
What The 2026 Medicare Financial Reset Means To Advanced Tissue Bioscience Companies... And What To Do About It.